INTRODUCTION
Circulating thrombocytes or platelets are anuclear discoid cells that are produced in the bone marrow from megakaryocytes during fragmentation. Thrombopoietin is the main growth factor controlling megakaryocyte production. The circulating life span of native platelets is approximately 10 days, and that of transfused platelets is approximately 3 days in a stable recipient. Platelets have receptors on their surface and granules inside, allowing them to participate in adhesion, aggregation and clot formation on the surface of injured endothelium, forming a haemostatic plug. The number of circulating platelets for an adult normally ranges between 150 × 109/L and 450 × 109/L. Decreased number of platelets (thrombocytopenia) refers to any situation where the patient’s platelet concentration is below 150 × 109/L, in an adult. Both thrombocytopenia and platelet dysfunction without thrombocytopenia can cause bleeding. Actively bleeding patients might require support from platelet transfusions. Platelets are also used for prophylactic transfusions to prevent bleeding due to decreased platelet production in patients undergoing chemotherapy, and/or haematopoietic stem cell transplantation (HSCT). In addition, platelets are transfused to some patients who have an increase in platelet destruction/consumption.
CAUSES OF THROMBOCYTOPENIA
Patients undergoing chemotherapy, HSCT, and those with chronic infections can have decreased platelet production. Another common cause of thrombocytopenia is an increase in platelet destruction/consumption that can have an immune or non-immune aetiology. Immune-mediated thrombocytopenia (ITP) is caused by different types of antibodies (autoimmune or alloimmune) that are produced to different platelet antigens and lead to elimination of the platelets in the spleen. Non-immune mechanisms cause platelet consumption and/or sequestration due to bleeding, enlarged spleen (sequestration) or vascular thrombi formation.
PROPHYLACTIC PLATELET TRANSFUSIONS
Prophylactic platelet transfusions in patients with hypoproliferative thrombocytopenia
Prophylactic platelet transfusions are routinely used in patients treated with chemotherapy and/or HSCT. They reduce the rate of spontaneous haemorrhagic events and improve clinical outcomes [1]. Although not yet a standard of practice, there is emerging evidence that prophylactic platelet transfusions are not necessary in autologous bone marrow transplant patients with hypoproliferative thrombocytopenia. The data suggest that this group of patients can be safely managed with therapeutic platelet transfusions only when bleeding occurs. The recommendation for prophylactic platelet transfusions in stable patients with hypoproliferative thrombocytopenia is to transfuse when the platelet count is 10 × 109/L or below. Multiple studies showed that, in stable patients with hypoproliferative thrombocytopenia, the platelet threshold above 10 × 109/L is adequate to minimize World Health Organization grade 2 or higher bleeding [2–4].
Prophylactic platelet transfusions in patients with dengue infection
Dengue infection is a major public health issue around the world, mainly in tropical and subtropical locations. Symptoms can vary from mild flu-like symptoms to more severe complications such as massive bleeding, shock and death. Thrombocytopenia is a common abnormal laboratory finding encountered in dengue infection, and bleeding is one of the complications that can occur. Different approaches, prophylactic versus therapeutic, have been studied in thrombocytopenic patients with dengue infection and the results are somewhat controversial. In addition, the optimal platelet threshold for prophylactic platelet transfusions is still being debated and evidence is still being generated in dengue patients [5]. However, at present, it is accepted that prophylactic transfusions should be given when the patient’s platelet count is 20 × 109/L or less [6,7], as platelet counts can decline very rapidly in this group of patients.
Prophylactic platelet transfusions in the setting of invasive procedures
Prophylactic platelet transfusions might be indicated in thrombocytopenic patients pre-procedure at specific platelet count triggers. They may also be required in patients with certain causes of platelet dysfunction, for example, aspirin, P2Y12 inhibitors (clopidogrel, prasugrel). There are multiple guidelines from different societies including multiple specialties (interventional radiology, thoracic surgery, haemostasis and thrombosis, haematology, blood transfusion) throughout the world on thresholds for prophylactic platelet transfusions for this group of patients. The established guidelines have some differences and there is some heterogeneity in the quality of evidence on which they are based but, overall, they are in line with each other. The recommended targeted thresholds for prophylactic platelet transfusions are listed below for some of the most common surgeries and procedures [9–13]. Platelet transfusions should be administered pre-procedure if platelet count falls below these targets:
- General surgery (nonneuraxial) < 50 × 109/L;
- Neurosurgery and ophthalmic surgery <100 × 109/L;
- Central venous catheter insertion < 20 × 109/L;
- Lumbar puncture < 50 × 109/L;
- Bone marrow biopsy < 20 × 109/L;
- Percutaneous liver biopsy < 50 × 109/L;
- Thorax centesis < 50 × 109/L.
Dose of prophylactic platelets
An adequate dose for prophylactic platelet transfusions is 1 apheresis unit or a dose of 4–5 pooled whole blood-derived platelet units for an average-size adult (70 kg). These doses result in a typical platelet increment in adults of 20,000–40,0000/μL. Apheresis platelets offer higher CCIs post-transfusion [8] but, overall, the two types of platelet products offer equivalent platelet survival and haemostatic effect in bleeding patients. In other words, higher CCIs with apheresis platelets do not translate into superior haemostatic effectiveness compared to whole blood-derived platelets.
One standard dose of platelets, either apheresis or a pool of whole blood-derived platelets, contains 3–4 × 1011 platelets on average. Interestingly, low (1.1 × 1011), medium (2.2 × 1011) and high doses (4.4 × 1011) of platelets transfused were equally effective in preventing bleeding in patients with hypoproliferative thrombocytopenia [3]. Patients in the low-dose category received platelet transfusions more frequently due to lower post-transfusion platelet increments compared to medium- and high-dose groups. High doses of platelets had no advantage in preventing bleeding compared to low- and medium-dose groups. In the study, the doses of platelets were adjusted for patient’s body surface area.
PLATELET TRANSFUSIONS IN THE BLEEDING PATIENT
Platelet transfusions can also be administered therapeutically for actively bleeding patients, but the optimal threshold for many settings is not known as few trials have addressed this issue. The typical platelet threshold for platelet transfusion in an actively bleeding patient is a platelet count below 50 × 109/L. In patients with cerebral haemorrhage, platelet transfusions should be given when platelet count is below 100 × 109/L. Independent of the platelet count, platelets should be administered to a bleeding patient with a known platelet dysfunction (such as a patient on antiplatelet medication or the surgery requires cardiopulmonary bypass). In addition, platelets are given in trauma resuscitation along with plasma and red blood cells, frequently as part of a major haemorrhage or massive transfusion protocol.
IDENTIFICATION AND MANAGEMENT OF PLATELET REFRACTORINESS
In patients, when a smaller than expected increase in the platelet count increment occurs after transfusion of an adequate dose of platelets, platelet refractoriness should be considered. One unit of random donor platelets derived from a unit of whole blood can increase the platelet count in an average size adult by 5,000–10,000/μL. Therefore, a dose of one random donor platelet per 10 kg of body weight is generally recommended. Pooled platelets prepared by pooling of 4–6 units of whole blood-derived platelets can give a post-transfusion increment of 20,000 to 40,000/μL in an average-size adult. The same increment would be expected from a dose of apheresis platelets.
There are two major causes of platelet refractoriness related to the patient: non-immune (80%) and immune (20%) causes. It is not uncommon to have a combination of both immune and non-immune causes.
When platelet refractoriness is suspected, a detailed review of the patient’s clinical history, along with a review of a history of platelet transfusions (how many transfusions and what increments were achieved), is indicated. To separate immune and non-immune causes of platelet refractoriness, a calculation of two consecutive CCIs is recommended. CCI is calculated 10–60 min post-platelet transfusion using the following formula:

BSA = body surface area
The formula uses number of platelets transfused and body surface area to adjust CCI for these parameters. CCIs that are <7,500 after two consecutive transfusions define the immune refractory state.
Rules for calculating CCI and an example of calculation:
- Two consecutive CCIs;
- 10–60 min post-transfusion;
- A patient with body surface area of 1.7 m2 received a unit of apheresis platelets containing 4 × 1011 platelets, a post-transfusion count rose from 10,000 to 30,000/μL.
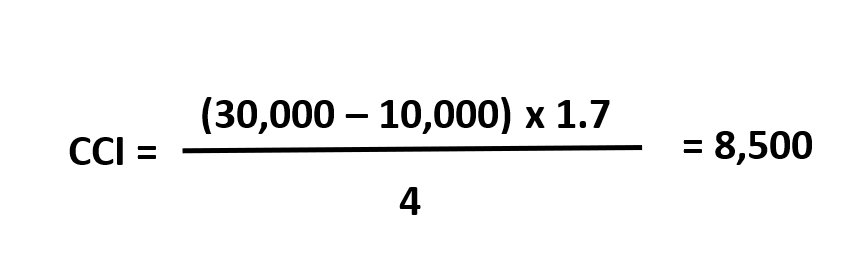
This is an example of CCI calculation. CCI is 8,500. The consecutive CCI is still 8,500. There is no evidence of immune refractoriness in this patient and non-immune causes should be considered.
While, overall, the major causes of platelet refractoriness are non-immune, the major immune cause of platelet refractoriness is HLA class I antibodies and they comprise approximately 90% of all immune causes. HLA antibody testing and HLA typing should be performed as part of the immune refractoriness evaluation. When HLA refractoriness is confirmed, HLA-matched platelets need to be obtained for future transfusion support, where these are available. HLA-matched platelets can only be collected by apheresis. HLA-A and HLA-B grade platelet matches provide the best platelet increments post-transfusion. Leucoreduction of blood components decreases the rate of HLA alloimmunization and the incidence of immune platelet refractoriness. Therefore, leucoreduced products should be transfused to patients requiring frequent transfusions, such as patients with haematological malignancy, HSCT and solid organ transplant recipients/candidates in order to prevent HLA alloimmunization.
Not all the HLA-matched platelet transfusions result in a successful post-transfusion platelet increment. In the majority of cases, the reason for that is overpowering non-immune mechanisms of platelet refractoriness. Therefore, immediate attention should be paid to these factors (splenomegaly, sepsis, fever, anti-fungal therapy, etc.) and appropriate therapeutic steps should be taken, if possible, to mitigate their impact on platelet refractoriness. Another reason for not responding to HLA-matched platelet transfusions may be the additional presence of HPA antibodies. Then, both HPA- and HLA-matched platelets may be necessary. As a temporary measure, while a search for HLA-matched platelets is still underway, providing transfusion support with whole blood-derived ABO-compatible platelets can be considered in case of bleeding.
Another technique that can be used to find compatible platelets in an HLA-alloimmunized recipient is the platelet crossmatch. Platelets from the platelet products are mixed with the patient’s plasma and compatible units are issued to the patient. This technique is fast and can be an effective alternative to HLA matching. However, it is not logistically feasible in highly immunized patients, since an extremely large number of platelet units would need to be crossmatched to find units that are compatible. Each of the techniques, HLA matching and crossmatching, has its advantages and disadvantages. The current evidence does not support the use of one technique over the other, and locally available resources are likely an important factor in determining which method will be utilized.
In an actively bleeding patient, when all the treatment options for non-immune causes of platelet refractoriness are exhausted and HLA-matched platelets are not available, other therapeutic options can be considered (antifibrinolytics, intravenous immunoglobulin) along with transfusions of non-HLA-matched platelets.
ABBREVIATIONS
CCI corrected count increment
DIC disseminated intravascular coagulation
HLA human leucocyte antigen
HPA human platelet antigen
HSCT haematopoietic stem cell transplantation
ITP immune thrombocytopenia
CONFLICT OF INTEREST STATEMENT
Alesia Kaplan: no disclaimers for this manuscript or conflict of interest.Darrell J. Triulzi: consultant to Fresenius Kabi.
Mark H. Yazer: no disclaimers for this manuscript or conflict of interest.
SUGGESTED READING
1.https://www.asco.org/practice-guidelines/quality-guidelines/guidelines/supportive-care-and-treatment-related-issues#/10171
2.http://www.aabb.org/programs/clinical/Pages/default.aspx
3.https://thorax.bmj.com/content/65/Suppl_2/i61
4.https://b-s-h.org.uk/guidelines/guidelines/use-of-platelet-transfusions/
5.https://www.brit-thoracic.org.uk/standards-of-care/guidelines/bts-guideline-for-diagnostic-flexible-bronchoscopy-in-adults/
REFERENCES
1. Stanworth SJ, Hudson CL, Estcourt LJ, Johnson RJ, Wood EM. Risk of bleeding and use of platelet transfusions in patients with hematologic malignancies: Recurrent event analysis. Haematologica. 2015;100:740–7.
2. Kumar A, Mhaskar R, Grossman BJ, Kaufman RM, Tobian AAR, Kleinman S, et al. Platelet transfusion: A systematic review of the clinical evidence. Transfusion. 2015;55:1116–27.
3. Slichter SJ, Kaufman RM, Assmann SF, McCullough J, Triulzi DJ, Strauss RG, et al. Dose of Prophylactic Platelet Transfusions and Prevention of Hemorrhage. N Engl J Med. 2010; 362:600–13.
4. Stanworth SJ, Estcourt LJ, Llewelyn CA, Murphy MF, Wood EM. Impact of prophylactic platelet transfusions on bleeding events in patients with hematologic malignancies: A subgroup analysis of a randomized trial (CME). Transfusion. 2014;54:2385–93.
5. Lee TH, Wong JGX, Leo YS, Thein TL, Ng EL, Lee LK, et al. Potential Harm of Prophylactic Platelet Transfusion in Adult Dengue Patients. PLoS Negl Trop Dis. 2016; 10:e0004576.
6. Makroo RN, Raina V, Kumar P, Kanth RK. Role of platelet transfusion in the management of dengue patients in a tertiary care hospital. Asian J Transfus Sci. 2007; 1:4–7.
7. Thomas L, Kaidomar S, Kerob-Bauchet B, Moravie V, Brouste Y, King JP, et al. Prospective observational study of low thresholds for platelet transfusion in adult dengue patients. Transfusion. 2009; 49: 1400–11.
8.Triulzi DJ, Assmann SF, Strauss RG, Ness PM, Hess JR, Kaufman RM, et al. The impact of platelet transfusion characteristics on posttransfusion platelet increments and clinical bleeding in patients with hypoproliferative thrombocytopenia. Blood. 2012; 119:5553–62.
9. Kaufman RM, Djulbegovic B, Gernsheimer T, Kleinman S, Tinmouth AT, Capocelli KE, et al. Platelet transfusion: A clinical practice guideline from the AABB. Ann Intern Med. 2015;162:205–13.
10. Havelock T, Teoh R, Laws D, Gleeson F. Pleural procedures and thoracic ultrasound: British Thoracic Society pleural disease guideline 2010. Thorax. 2010;65(Suppl. 2):61–76.
11. Schiffer BCA, Anderson KC, Bennett CL, Bernstein S, Elting LS, Goldsmith M, et al. Platelet Transfusion for Patients With Cancer: Clinical Practice Guidelines of the American Society of Clinical Oncology. J Clin Oncol. 2016;19:1519–38.
12. Estcourt LJ, Birchall J, Allard S, Bassey SJ, Hersey P, Kerr JP, et al. Guidelines for the use of platelet transfusions. Br J Haematol. 2017;176:365–94.
13. Du Rand IA, Blaikley J, Booton R, Chaudhuri N, Gupta V, Khalid S, et al. British Thoracic Society guideline for diagnostic flexible bronchoscopy in adults. Thorax. 2013;68(Suppl. 1): i1–i44.
RESOURCES

THE AUTHORS

Alesia Kaplan
Dr. Kaplan is an Assistant Medical Director of a large Centralized Transfusion Service (CTS), Clinical Services Vitalant-Pittsburgh that provides clinical transfusion support to the UPMC health system hospitals. Dr. Kaplan is committed to research and to teaching medical technologists, medical students, residents and fellows.
Clinical Expertise
Dr. Kaplan has general expertise in transfusion medicine with particular interest in Patient Blood Management. Dr. Kaplan is responsible for the HIV/HCV lookback program.
Education & Training
MD - Vitebsk State Medical University, Belarus, 2006
AP/CP Residency - University of Minnesota, 2014
BB/Transfusion Medicine Fellowship - University of Minnesota, 2015
Awards
2014 University of Minnesota, Pathology, Ernst Award for Research
2016 and 2018 Best CP Teacher of the Year Award, University of Pittsburgh
Research Interests
Dr. Kaplan's research interests include Pathogen Inactivation Technologies for blood products and Patient Blood management. Dr. Kaplan is currently a primary investigator on the study sponsored by Cerus corporation looking at transfusion of pathogen inactivated RBCs in cardiac surgery patients. Dr. Kaplan is working on two cold stored platelet clinical trials: Department of defense (DOD) funded Chilled Platelet Study (CHIPS)) trial in adult and pediatric patients undergoing cardiothoracic surgery and department of defense (DOD) funded Cold Stored Platelets Early Intervention-Traumatic Brain Injury (TBI) trial (CriSP-TBI). Dr. Kaplan participated as a co-investigator in an NIH funded Clinical Trial of COVID-19 Convalescent Plasma in Outpatients (C3PO).
Representative Publications
- Seheult JN, Tysarczyk M, Kaplan A, Triulzi DJ, Yazer MH. Optimizing blood bank resources when implementing a low-titer group O+ whole blood program: an in silico study. Transfusion. 2020 Aug;60(8):1793-1803.
- Smith JA, Seheult JN, Sevcik J, Kiss JE, Kaplan A. Process mapping of the urgent red cell exchange procedure for patients with severe complications of sickle cell disease at a centralized hemapheresis service. J Clin Apher. 2020 Sep;35(5):427-434.
- Seheult JN, Stram MN, Sevcik J, Kaplan A, Kiss JE. Benchmarking the centralized urgent plasma exchange service for patients admitted with a diagnosis of suspected acquired thrombotic thrombocytopenic purpura at a large healthcare system. J Clin Apher. 2021 Jun 25. doi: 10.1002/jca.21916. Epub ahead of print.
- Korley FK, Durkalski-Mauldin V, Yeatts SD, Schulman K, Davenport RD, Dumont LJ, El Kassar N, Foster LD, Hah JM, Jaiswal S, Kaplan A, Lowell E, McDyer JF, Quinn J, Triulzi DJ, Van Huysen C, Stevenson VLW, Yadav K, Jones CW, Kea B, Burnett A, Reynolds JC, Greineder CF, Haas NL, Beiser DG, Silbergleit R, Barsan W, Callaway CW; SIREN-C3PO Investigators. Early Convalescent Plasma for High-Risk Outpatients with Covid-19. N Engl J Med. 2021 Aug 18:NEJMoa2103784. doi: 10.1056/NEJMoa2103784. Epub ahead of print.
- Bubar R, Kiss JE, Triulzi DJ, D'Andrea P, Zilich A, Kaplan A. How do we…consistently provide high-dose granulocyte products for transfusions in neutropenic patients? Transfusion. 2023 Jul;63(7):1267-1276.
- Thant M, Cancelas J, Kaplan A. The enhanced direct antiglobulin test in current practice has a limited impact on management of adult patients. Transfus Apher Sci. 2023 Aug 17:103768.
Darrell J. Triulzi
Dr. Triulzi is the Director of the Division of Transfusion Medicine, Department of Pathology and Medical Director, Clinical Services Vitalant-Pittsburgh. Dr Triulzi serves as the division leader in transfusion medicine. The division provides clinical transfusion support to the UPMC health system hospitals and is actively involved in its Patient Blood Management Program. Dr Triulzi leads a robust clinical research program in the division.
Clinical Expertise
Dr. Triulzi has general expertise in the area of transfusion medicine with particular clinical and research expertise in transfusion support of oncology/hematology, trauma, cardiac surgery and organ and stem cell transplant patients. He is highly involved both locally and nationally in Patient Blood Management and its application to orthopedic surgery, cardiac surgery and trauma.
Education & Training
MD - Albany Medical College, 1985
Internship - Internal Medicine University of Pittsburgh, 1986
Residency - Anatomic and Clinical Pathology, 1990
Fellowship - Blood Bank/Transfusion Medicine, Johns Hopkins, 1992
Research Interests
Dr. Triulzi's research interests include red cell storage, platelet transfusions, transfusion related acute lung injury (TRALI), transfusion associated circulatory overload (TACO), leukoreduction, and transfusion support of stem cell and solid organ transplant recipients. The Division participates in multi-institutional NIH funded clinical trials in transfusion medicine and hemostatsis including MINT, A-TREAT, PPOWER and SCD CARRE. Dr Triulzi also served as the PI on the REDSIII NHLBI epidemiologic study of recipient outcomes and donor safety (REDSIII). Current areas of investigation include red cell transfusion triggers, anti-fibrinolytic therapy in adult and pediatric hematology-oncology patients and red cell exchange in patients with sickle cell disease.
NIH Research
View Dr. Triulzi's NIH RePORT on nih.gov
Representative Publications
View Dr. Triulzi's publications on PubMed
Carson JL, Triulzi DJ, Ness PM. Indications for and Adverse Effects of Red-Cell Transfusion. N Engl J Med. 2017 Sep 28;377(13):1261-1272. doi: 10.1056/NEJMra1612789. Review. No abstract available. PMID: 28953438.
Roubinian NH, Hendrickson JE, Triulzi DJ et al. Contemporary risk factors and outcomes of transfusion associated circulatory overload. Crit Care Med 2018;46:577-85. PMID: 29300236.
Leeper CM, Yazer MY, Cladis FP, Sladino R, Triulzi DJ, Gaines BA. Use of un-crossmatched cold-stored whole blood in injured children with hemorrhagic shock. (research letter).JAMA Pediatrics 2018 (on-line March 19, 2018).
Yazer MH, Cap AP, Spinella PC, Alarcon L, Triulzi DJ. How do I implement a whole blood program for massively bleeding patients? Transfusion 2018;58:622-628. PMID: 29332316.
Matthew S. Karafin MS, Westlake M, Hauser RG, Tormey CA, Norris PJ, Roubinian NH, Wu Y, Triulzi DJ, Kleinman S, Hendrickson JE. Risk factors for red blood cell alloimmunization in the Recipient Epidemiology and Donor Evaluation Study (REDS-III) database. Brit J Haem 2018;181:672-81. PMID: 29675950.
Seheult JN, Bahr M, Anto V, Alarcon LH, Corcos A, Sperry JL, Triulzi DJ, Yazer MH. Safety profile of uncrossmatched, cold stored, low-titer, group O+ whole blood in civilian trauma patients. Transfusion 2018;58: 2280-2288. PMID: 29802644.
Campbell-Lee SA, Gvozdjan K, Choi KM, Chen YF, Saraf SL, Hsu LL, Gordeuk VR, Strauss RG, Triulzi DJ. Red blood cell alloimmunization in sickle cell disease: assessment of transfusion protocols during two time periods. Transfusion 2018;58:1588-1596. PMID: 29570817.
Seheult JN, Anto V, Alarcon LH, Sperry JL, Triulzi DJ, Yazer MH. Clinical outcomes among low-titer group O whole blood recipients compared to recipients of conventional components in civilian trauma resuscitation. Transfusion 2018 Aug;58(8):1838-1845. PMID: 30160310.
Karafin MS, Tan S, Tormey CA, Spencer BR, Hauser RG, Norris PJ, Roubinian NH, Wu Y, Triulzi DJ, Kleinman SK, Gottschall JL, Hendrickson JE. Prevalence and risk factors for RBC alloantibodies in blood donors in the Recipient Epidemiology and Donor Evaluation Study-III (REDS-III). Transfusion 2019 Jan;59(1):217-225. PMID: 30427537.
Seheult JN, Stram MN, Sperry J, Spinella PC, Triulzi DJ, Yazer MH. In silico model of the dilutional effects of conventional component therapy versus whole blood in the management of massively bleeding adult trauma patients. Transfusion 2019 Jan;59(1):146-158. PMID: 30414181.









